
My colleagues and I were responsible for the animal studies and data analysis that subjected our nanoparticle formulation to its most important test. Here is what those experiments involved—and what they meant to me.
I am Umair Wahedi, co-author of the paper “Oral delivery of solid lipid nanoparticles surface decorated with hyaluronic acid and bovine serum albumin: A novel approach to treat colon cancer through active targeting,” published in the International Journal of Biological Macromolecules (2024). My specific contributions to this research were the in vivo animal studies, the data analysis, and participation in the overall conceptualisation of the study design. This is my perspective on what that work involved—and why it mattered.
Every research paper represents a team. My colleagues, Dr Syed Suhaib Ahmed, Dr Mohd Zubair Baba, and the wider group at JSS College of Pharmacy handled formulation chemistry, surface engineering, and cell culture experiments. My role was to take what they had built in the laboratory and ask the hardest question of all: Does it actually work inside a living body?
That question—does it work in vivo? —is where most drug delivery research either finds its legs or loses them. A nanoparticle that performs beautifully in a cell culture dish may behave entirely differently when it encounters the full complexity of a gastrointestinal tract, an immune system, and a living tumour. My job was to find out.
The Thinking behind the Design: Conceptualisation
Before any animal entered a study, there were months of thinking about the right experimental framework. Conceptualisation—which I contributed to alongside our team and under the guidance of Prof. Jawahar Natarajan—meant asking: what do we need to prove, and what is the most rigorous way to prove it?
We knew from the literature that 1, 2-dimethylhydrazine (DMH) is one of the most validated chemical carcinogens for inducing colorectal tumours in rats. It closely mimics the sequential stages of human colon carcinogenesis—from normal mucosa, through dysplasia, to frank malignancy. We chose it deliberately because we did not want results from an easy model. We wanted results from a model that would genuinely challenge our formulation.
The study was designed with five groups to allow for proper comparative interpretation. Every group had a specific purpose in the overall argument we were building about efficacy.
Group 1—Control → untreated rats—establishing what healthy colon biology looks like
Group 2—DMH Induced → Cancer induced, no treatment—the disease baseline
Group 3—Pure Drugs → IRN + DZN as free drugs—does the drug combination work without a nanocarrier?
Group 4—Unconjugated SLNs → Nanoparticle without surface targeting—isolating the targeting effect
Group 5—Conjugated SLNs ✦ → our full HA-BSA-chitosan formulation—the complete hypothesis
This layered design was critical. Without Groups 3 and 4, we could never confidently attribute our results to the nanoparticle system-specific. Every control group was a logical step in a chain of evidence.
This layered design was critical. Without Groups 3 and 4, we could never confidently attribute our results to the nanoparticle system-specific. Every control group was a logical step in a chain of evidence.
The Animal Study: What We Actually Did
Thirty male Albino Wistar rats, aged 5–6 weeks, were housed under controlled conditions—23 ± 2 °C, a 12-hour light-dark cycle, ad libitum access to food and water—and allowed a full week of acclimatisation before any intervention began. Animal welfare and ethical conduct were central throughout; the protocol was approved by the Institutional Animal Ethics Committee (IAEC) at JSSCP under registration with CPCSEA, and we followed ARRIVE guidelines for animal research reporting.
Day 1—Week 1
• Acclimatisation
Animals were allowed to settle into their environment. Body weight was recorded as a baseline. This week matters—stressed animals produce unreliable data, and we wanted the biology to be as clean as possible before we introduced any variables.
Weeks 1–16 • Induction Period
• DMH Administration—Building the Disease Model
Groups 2–5 received subcutaneous injections of DMH at 20 mg/kg, twice weekly for 16 weeks. This dose and schedule, drawn from the established literature, reliably induces colorectal adenocarcinomas. Weekly body weight monitoring let us track how the cancer was affecting overall health across groups.
Weeks 18–26 • Treatment Period
• Oral Drug Administration—Testing the Formulation
Treatment groups received their respective formulations orally, twice weekly for two months. Group 3 received pure IRN (10 mg/kg) + DZN (25 mg/kg). Groups 4 and 5 received unconjugated and conjugated SLNs respectively, both at 35 mg/kg. The oral route was a deliberate choice—it reflects real-world patient administration and is the most practically meaningful test of a targeted oral delivery system.
Day 187 • Termination
• Tissue Collection and Analysis
At study completion, colon tissues were harvested for histopathology, immunohistochemistry, and RT-PCR gene expression analysis. This is where the story of the formulation becomes visible at the tissue and molecular level.
The Data: Reading What the Animals Were Telling Us
Data analysis was not just number-crunching for me—it was the process of translating biological signals into a coherent scientific argument. Here is what we found, and what each finding meant.
Gene Expression—RT-PCR
We looked at two key molecular markers. Carcinoembryonic antigen (CEA) is a non-specific biomarker that surges in colorectal cancer—elevated CEA is one of the first things oncologists look for when monitoring colon cancer progression or recurrence. In our DMH-induced animals, CEA was significantly elevated compared to healthy controls. In animals treated with our conjugated SLNs, CEA expression showed a significant two-fold downregulation—a clear signal that tumour biology was being meaningfully suppressed.
TNF-α told the complementary story. This pro-inflammatory cytokine, produced by macrophages and immune cells, plays an important role in anti-tumour immunity. The treated groups showed significant upregulation of TNF-α—their immune systems were more actively engaged against the tumour. These two findings together painted a coherent picture: the formulation was reducing tumour burden and re-engaging the immune system simultaneously.

Figure 1 • From Our Paper:
RT-PCR gene expression results showing CEA and TNF-α mRNA levels across all five groups. Group 1: Control; Group 2: DMH induced; Group 3: unconjugated SLNs; Group 4: conjugated SLNs. CEA downregulation and TNF-α upregulation in treated groups confirm anti-tumour activity at the molecular level. (Ahmed et al., 2024, Fig. 16).
Histopathology—What the Tissue Showed
If the gene expression data were the molecular story, histopathology was the visual proof. We graded colon tissue sections by severity of dysplasia: mild, moderate, and severe. The DMH-induced group showed all the hallmarks of advanced colorectal pathology—ulcerated mucosa, distorted glands, elongated pleomorphic nuclei, loss of goblet cells, inflammatory infiltrates, and destruction of the muscularis mucosa. It was, at the cellular level, a textbook colon tumour.
The conjugated SLN-treated group showed something I found genuinely striking when I reviewed the slides. The mucosal architecture was restored. Normal goblet cells were present. The muscularis layers were intact. There were scattered mitotic figures—evidence of cellular activity—but the tissue overall looked close to healthy. For a formulation administered orally, reaching the colon through the entire gastrointestinal tract, and producing this degree of tissue restoration—that was a meaningful result.
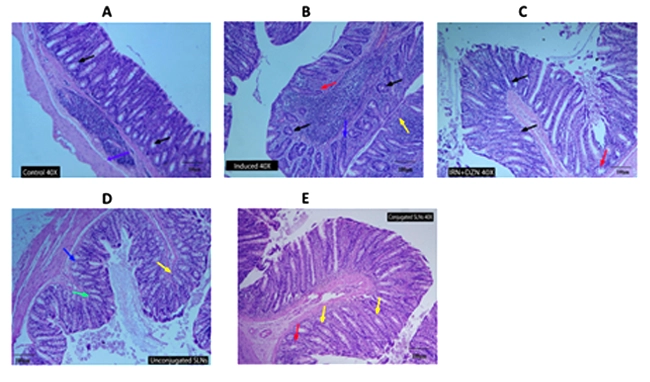
Figure 2 • From Our Paper
H&E-stained colon sections at 40× magnification: (A) Control—normal mucosal architecture; (B) DMH-induced—distorted glands, pleomorphic nuclei, goblet cell depletion; (C) Pure drugs—mild improvement; (D) Unconjugated SLNs—partial restoration; (E) Conjugated SLNs—near-normal mucosa with intact goblet cells and mucosal layers. (Ahmed et al., 2024, Fig. 17).
Ki-67 Immunohistochemistry—Measuring Proliferation
Ki-67 is a nuclear protein expressed only in actively dividing cells. High Ki-67 in colon tissue means uncontrolled proliferation—the fundamental engine of tumour growth. In our DMH-induced animals, Ki-67 staining was dramatically elevated compared to controls. In the conjugated SLN-treated group, Ki-67 expression was significantly attenuated, comparable to the unconjugated SLN group, and substantially lower than the disease group. The cancer cells were no longer multiplying at the same rate.
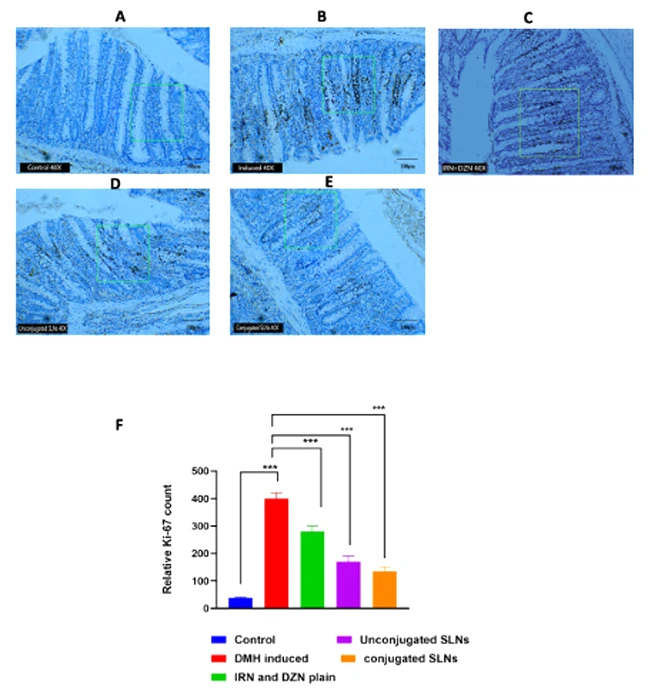
Figure 3: From our Paper
Immunochemical analysis of ki-67 expression (A) The control group showed a standard expression of Ki-67 under light microscopy. (B) The DMH-treated control group showed a robust expression of Ki-67. (C) IRN+ DZN pure drugs showed mild expression of ki-67; (D) unconjugated and (E) conjugated SLNs groups showed mild expression of ki-67. Magnification 40×. (F) The relative content of ki-67 in the immunochemical slides of colon tissue of the different experimental groups. (Ahmed et al., 2024, Fig. 18).
Statistical Analysis
All in vivo data were expressed as Mean ± SEM. I used two-way ANOVA followed by the Bonferroni post-hoc test for multiple group comparisons in the cell-level studies, and one-way ANOVA with Dunnet’s test for gene expression comparisons. Statistical significance was set at p < 0.05 throughout. Every result reported in the paper passed this threshold. The Ki-67 IHC analysis used ImageJ Fiji software for semi-quantitative pixel density measurement across 10 randomly selected fields per slide—a method chosen to reduce subjectivity in what is inherently a visual assay.
The moment the histopathology slides came back, and I could see—visually, unmistakably—that the treated colon tissue had recovered its normal architecture, I knew the in vivo data was telling a coherent story. Numbers confirm it. Tissue sections show it.
What Made This Conceptually Different
From the conceptualisation standpoint, what I think distinguishes this study is the integration of passive and active targeting in a single oral formulation. Most nanoparticle cancer research focuses on intravenous delivery—you inject the formulation directly into the bloodstream, bypassing all the challenges of the gastrointestinal environment. Oral delivery is far harder. The formulation must survive the stomach’s acidity, the enzymatic environment of the small intestine, and the mucus barrier of the colon—before it can even attempt to reach a tumour.
Our chitosan outer coating addresses the GI survival problem. The HA-BSA targeting coat addresses the selective uptake problem. Together, the design is built for the oral route from the ground up—not retrofitted to it. That was a deliberate conceptual choice, and the in vivo data validated it.
Why in-vivo Evidence Is the Hardest—and Most Important—Kind
Cell culture is essential for mechanistic understanding, but it cannot replicate the immune system, the microbiome, hepatic first-pass metabolism, or the physical architecture of a real tumour with its surrounding stroma and vasculature. An in-vivo study does not just test a drug—it tests an entire biological system. That is why it is both the most demanding and the most convincing form of evidence we can produce at the preclinical stage.
Limitations I Want to Be Honest About
Good data analysis means being as clear about what you did not prove as what you did. Our animal model, while well-validated, uses a chemical carcinogen to induce cancer, which is not identical to spontaneous human colorectal cancer with its genetic heterogeneity. The study was conducted in male Wistar rats only; sex differences in drug response are a well-documented phenomenon, and our data cannot speak to female biology. The treatment period of two months, while adequate for proof-of-concept, is shorter than the duration of real colon cancer treatment in humans.
These are not weaknesses to hide—they are honest boundaries on the claims we make. Preclinical in vivo evidence is a necessary but not sufficient step. Human pharmacokinetics, safety profiles, and dose optimisation all require clinical investigation that lies ahead.
A Word on the Team
Research of this scope does not come from one person. The in-vivo findings Dr. Mohd Zubair Baba and I contributed would have meant nothing without the formulation that Syed Suhaib Ahmed and the pharmaceutics team engineered, or the chemical characterisation work contributed Jayanthi Koppula, or the pharmacology expertise of Dr. Divakar Selvaraj. Prof. Jawahar Natarajan’s supervision gave the entire project its scientific rigour and strategic direction.
My role was to make sure that what was built in the lab could survive contact with living biology. I believe the data shows it can. That gives me genuine confidence that this direction of research—oral targeted nanoparticles combining natural and synthetic therapeutics—deserves to be pursued further.
Umair Wahedi
Research Assistant, SEMRC
Co-author Department of Pharmaceutical Chemistry
JSS College of Pharmacy, JSS Academy of Higher Education & Research, Ooty, Tamil Nadu
Contributed to in vivo study design and execution, statistical data analysis, and conceptualisation of the overall research framework. Research conducted under the supervision of Prof. Jawahar Natarajan with institutional support from DST-FIST, DST-PURSE, and DBT-BUILDER programmes.
Full Citation:
Syed Suhaib Ahmed, Mohd Zubair Baba, Umair Wahedi, Jayanthi Koppula, Murthannagari Vivek Reddy, Divakar Selvaraj, Senthil Venkatachalam, Jubie Selvaraj, Veintramuthu Sankar, Jawahar Natarajan. “Oral delivery of solid lipid nanoparticles surface decorated with hyaluronic acid and bovine serum albumin: A novel approach to treat colon cancer through active targeting.” International Journal of Biological Macromolecules, 2024.
Leave A Comment